|
CEREBRAL PALSY AND STRENGTH TRAINING:
BENEFICIAL OR NOT
by Lori
Ann Bruns; University of Florida,
Graduate Level Distance Education Student;
Owner of Curves Fitness Center
INTRODUCTION
Strength
training is a vital component of a fitness
program. Many people consider strength
training as something only athletes
partake in, but strength is something
necessary for life. Without strength,
moving, walking, talking, eating, or
even breathing would be impossible (Koscielny,
n.d.).
In the last
few decades more is becoming known about
the benefits of muscle strength and
endurance ("Strength
Training," 2006). Research
over past years has found that strength
development is a vital part of most
health and fitness programs (Kraemer,
2003). A study by Winett &
Carpinelli (2001) demonstrates that
strength training has enormous effects
on the musculoskeletal system, assists
with the maintenance of functional capabilities,
and has the ability to prevent osteoporosis,
sarcopenia,
pain of the lower back, and other disabilities.
 Some
recent influential studies show that
resistance training may also play a
role in resting metabolic rate, body
fat, blood pressure, gastrointestinal
transit time, which are closely linked
with heart disease, cancer, and diabetes
(Winett &
Carpinelli). Studies by Ebben
& Jensen (1998);
Fleck (1998);
Freedson (2000)
established that a strength training
program can have both physiological
and psychological benefits, for both
men and women (as
cited by Harne & Bixby 2005),
but what about men and women who have
cerebral palsy? Some
recent influential studies show that
resistance training may also play a
role in resting metabolic rate, body
fat, blood pressure, gastrointestinal
transit time, which are closely linked
with heart disease, cancer, and diabetes
(Winett &
Carpinelli). Studies by Ebben
& Jensen (1998);
Fleck (1998);
Freedson (2000)
established that a strength training
program can have both physiological
and psychological benefits, for both
men and women (as
cited by Harne & Bixby 2005),
but what about men and women who have
cerebral palsy?
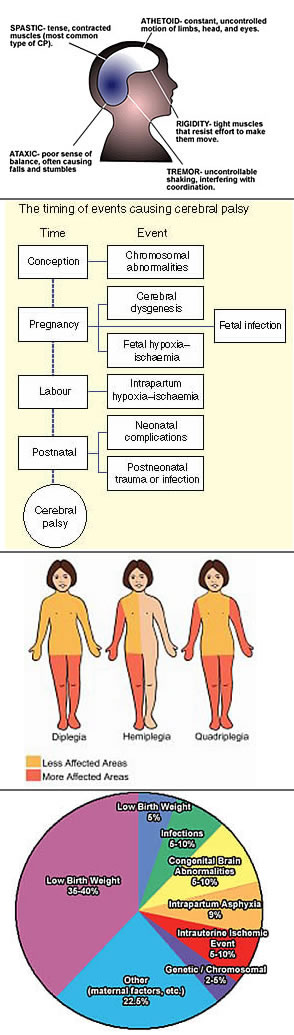
Cerebral
palsy (CP) is "a group of permanent
disabling symptoms resulting from damage
to the motor control areas of the brain…manifesting
itself in a loss or impairment of control
over voluntary musculature" (Winnick,
2005, p. 236). Cerebral palsy
is the most common cause of physical
disability in children with two out
of every 1,000 live births in the United
States (Lehman,
Garban, Scott, Tant, & White, 2008).
For years there has been hesitation
in the therapy world as to whether or
not strength testing and training should
be performed on people with cerebral
palsy, while some physical educators
and people in the medical field haven't
agreed with this perspective (Damiano,
Dodd, & Taylor, 2002).
Recently
a literature review was published refuting
the effectiveness of muscle strengthening
in children with cerebral palsy (Scainni,
Butler, Ada, & Teixeira-Salmela,
2009), going against previous
literature reviews by Darrah, Fran,
Chen, Nunweiler, & Watkins (1997),
Haney (1998),
Dodd, Taylor & Damiano et al. (2002),
and most currently, Verschuren, Ketelaar,
Takken, Helder, & Gorter (2007).
The reasons why strength training isn't
widely used by many physical therapists
are multifaceted (Damiano
et al.). The lack of strength
gains, increases in spasticity, and
inability to perform strength exercises
due to movement controlled by chained
reflexes were some of the reasons why
there was a believe that people with
cerebral palsy should not strength train
(Damiano et al.).
Due to such conflicting reviews it is
necessary to reexamine the topic of
whether or not strength training for
people with cerebral palsy is beneficial
or not.
CEREBRAL
PALSY AND MUSCLE STRENGTH, MOBILITY,
AND GAIT FUNCTION
"Our
bodies are miracles of adaptability,
capable of altering themselves in response
to loads placed upon them in such a
way that future, similar loads will
be less stressful. Likewise, they can
and will adapt to having no demands
placed upon them, becoming increasingly
weaker and less capable" (Strength
Training, 2006, para. 8). Bartlett
& Palisano (2002)
concluded that muscle strength, not
spasticity, is a main impairment that
plays a role in motor functioning in
children with cerebral palsy. Damiano
et al. (2002)
and Eagleton, Iams, McDoell, Morrison,
& Even (2004)
also agreed that muscle weakness significantly
decreases ambulation. Some therapists
are not eager to strength train people
with cerebral palsy due to the lack
of sufficient strength gains (Damiano
et al.) and no evidence of improvements
in activity (Scianni
et al., 2009).
A study done
by Scholtes et al. (2010)
evaluated functional progressive
resistance exercise strength training
on mobility and muscle strength in children
with cerebral palsy. Fifty-one children
with uni- and bilateral spastic cerebral
palsy were placed in either the intervention
group, which consisted of 12 weeks of
progressive circuit training, or the
control group, receiving usual care.
Muscle strength and mobility were all
measured before, during, directly after,
and six weeks after the training had
ended. The results showed a significant
change in muscle strength.
Knee extensor
strength increased by 12 percent and
hip abductor strength increased by 11
percent, while six-repetition leg-press
maximum increased by 14 percent. Despite
all the significant increases in strength,
no changes were observed in mobility.
The researchers stated that a probable
cause for not observing an increase
in mobility was because the improvements
in strength weren't enough in order
to improve mobility. Another suggestion
may have been that the number of each
individual muscle that increased in
strength was too limited (Scholtes
et al.).
To some extent
the results of the Scholtes et al. 2010
study coincide with the findings of
Damiano, Arnold, Steele, & Delp
(2010).
The aim of this study was to determine
if strength training could decrease
the extent of crouched, internally rotated
gait in children with cerebral palsy.
Eight children followed an eight-week
progressive resistance program. Measures
were taken before and after the program
in three-dimensional gait
analysis and isokinetic
testing. The results showed that the
left hip extensors had significant changes
in strength going from 10.7 ft-lb to
19.2 ft-lb (p=0.01), which is a 79.4%
change. The right hip extensors and
right and left knee extensors all increased
as well, but non-significantly. In terms
of gait
kinematics,
some but not all of the children improved
with hip and knee extension.
Stride length,
cadence,
and gait speed were not significantly
different from the pre measures, and
the increases that were seen varied
among each individual. The researchers
concluded that strength training may
have the ability to improve walking
function and alignment in some people
with cerebral palsy when weakness is
a big contributor to the deficits in
gait. Furthermore, there may also be
no change or even undesired results
in other patients. A larger sample size
is needed in order to determine validity
of this study.
These findings
contradict the findings of Morton, Brownlee,
& McFadyn (2005),
Eagleton et al. (2004),
Blundell, Shephard, Dean, & Adams
(2003), Nystrom Eek, Tranberg, Zugner,
Alkema, & Beckung (2008)
and Andersson, Grooten, Hellsten, Kaping,
& Mattsson (2003).
In the pilot study by Morton et al.,
eight children with cerebral palsy underwent
a six-week progressive training session,
which included strength training three
times a week.
Measurements
were taken at the beginning, immediately
after, and again after a four-week follow
up. There was a statistically significant
result in the quadriceps and hamstrings
mean strength. As far as the gait results,
self-selected mean walking speed went
from 0.55 m/s to 0.67 m/s post training
and then to 0.62 m/s at the follow-up.
Fast walking speed also increased going
from 0.55 m/s to 0.67 m/s after the
training to 0.62 m/s. Self-selected
cadence increased from 93.96 steps/min
to 108.87 steps/min to 105.64 steps/min.
Fast cadence also increased after the
strength training intervention, and
then decreased following four weeks.
Self-selected step length went from
0.34 m to 0.37 m back down to 0.34 m
at the follow-up. Fast step length also
showed the same changes of an increase
followed by a decrease at the follow-up.
Eagleton et al. examined trunk and lower
body muscle strength as well as gait
velocity, step length, and cadence.
The researchers
recruited seven adolescents with cerebral
palsy to participate in a six-week intervention
of strength training. The findings showed
that all five variables increased significantly.
As a result, the researchers concluded
that resistance raining is an important
form of physical therapy for children
with cerebral palsy.
Blundell et al. (2003)
examined eight children between the
ages of four and eight, with cerebral
palsy, who participated in a training
program that lasted four weeks. The
participants underwent exercises that
were similar to daily tasks in order
to increase functional ability. The
activities included picking up objects
from a couched position to increase
balance, step-ups and step-downs, sit-to-stand
and leg press for strength, and walking
on treadmills, as well as up and down
ramps and stairs. Each session of strength
training was an hour long and two times
a week, with intensity being increased
gradually. After four weeks, not only
were there improvements in muscle strength,
but in functional ability as well. Hip
flexors and extensors, dorsiflexors,
and knee extensors all showed significant
increases in strength and the functional
test in the step-ups, minimum chair
height test, timed walk, and stride
length increased significantly as well.
Eight weeks following the training period,
the improvements were still visible.
Nystrom Eek
et al. (2008)
investigated the influence of strength
training on gait in children with cerebral
palsy. Three days a week for eight weeks,
sixteen children participated in lower
body resistance training including free
weights, rubber bands, and body weight.
At the beginning of training, measurements
were taken in Gross Motor Function
Measure (GMFM)
assessment, joint range of motion assessment,
as well as three-dimensional gait analysis.
After the training period, there were
significant increases in muscle strength
in the knee flexors and hip muscle groups.
There was also a significant increase
in GMFM as well as stride length, but
no significance in gait velocity and
a decrease in cadence after training.
The researchers
concluded that a resistance-training
program increased strength and improved
gait function in children with cerebral
palsy. Andersson et al. (2003)
examined the effects of progressive
strength training on seven individuals
with cerebral palsy, while three were
placed in the control group. After ten
weeks of training twice a week, significant
improvements were seen in isometric
strength (hip extensors p=0.006; hip
abductor p=0.01), isokinetic concentric
work (knee extensors p=0.02). There
were also statistically significant
increases in GMFM (p=0.005) Timed "Up
and Go" test (p=0.01), and walking
velocity (p=0.005). Ross & Engsberg
(2007)
found that spasticity was not related
to gait and motor function, but strength
was highly related to motor function.
Salem &
Godwin (2009)
also went against the findings by Scholtes
et al. (2010),
but along with Blundall et al (2003).
Salem & Godwin examined ten children
with cerebral palsy to assess mobility
after task-oriented strength training.
Five children were assigned to the experimental
group, and five were in the control
group. The children placed in the experimental
group received task-oriented resistance
training focusing on lower body strengthening,
while the children in the control group
focused on improving balance through
reinforcement and normalization of movement
patterns through conventional physical
therapy (Salem
& Godwin). Mobility was measured
using the Gross Motor Function Measure
and the Timed "Up and Go"
test.
After the
five-week session came to an end the
researchers found there were significant
improvements in mobility in the experimental
group. The experimental group significantly
lowered the time to complete the Timed
"Up and Go" test (p=0.017).
Along those same experimental lines,
a study by Andersson et al. (2003)
showed that there were significant improvements
not only in strength, but GMFM and Timed
"Up and Go" test as well.
A similar
study done by Yan, Wang, Lin, Chu, &
Chan (2006)
examined task-oriented progressive resistance
strength and mobility in people with
stroke. Stroke in children often results
in a movement disorder very similar
to that resulting from cerebral palsy
("Cerebral
Palsy," n.d.). The two are
quite similar to each other, making
it important to analyze the studies
done with individuals with stroke as
well. Forty- eight individuals, a year
following a stroke, were either placed
in a control group or the experimental
group. The experimental group underwent
four weeks of task-oriented progressive
strength training while the control
group didn't do any kind of rehabilitation.
After the four weeks, measures were
taken in lower body muscle strength,
cadence, stride, gait velocity, length
of the stride, step test, six-minute
walk test, as well as the Timed "Up
and Go" test.
In the experimental
group, muscle strength significantly
in the strong side, which ranged from
23.9% to 36.5% as well as the paretic
side, ranging from 10.1% to 77.9%. The
control group had changes ranging from
a 6.7% increase to 11.2% decline. In
all of the measures that were examined,
the experimental group showed significant
improvements, while the control group
showed no changes in the measures except
for a significant decline of 20.3% in
the step test. There was a significant
association between the strength gain
and the gain in all the functional tests
in the experimental group. The results
from this study show that task-oriented
strength training may have the potential
to increase lower body strength as well
as functional mobility for people with
stroke, which could translate to people
with cerebral palsy.
Based on
this evidence, the evidence shows that
strength training it may need to be
task-oriented or progressive in nature
in order to see any improvement in mobility
function. Functional training that is
done to mimic everyday tasks, or strength
exercises specific for increasing muscles
used daily, seems to have the best result
according to Blundell et al. (2003)
and Salem & Godwin (2009).
SPASTICITY
There are
many different types of cerebral palsy,
with spastic
cerebral palsy being the most common
(Lehman et al.,
2008). One area of concern for
some physical therapists is the fear
of increasing spasticity because of
the great effort used in strength training.
"The Bobath neurodevelopmental
treatment approach advised against the
use of resistive exercise, as proponents
felt that increased effort would increase
spasticity" (Fowler
et al., p. 1215). Since the development
of that theory there has been advocates
against strength training due to increases
in spasticity despite studies showing
a lack of evidence in increased spasticity
(Scholtes et al.,
2010; Eagleton et al., 2004; Fowler
et al., 2001).
The study
by Andersson et al. (2003)
examined mobility in adults with cerebral
palsy, and spasticity as well. The study
showed that there were significant improvements
in muscle strength without increasing
spasticity. Fowler et al. (2001)
specifically examined whether or not
performance of exercises with maximum
efforts would increase spasticity in
people with cerebral palsy. Twenty-four
participants with cerebral palsy performed
three different forms of quadriceps
femoris exercises (isometric, isotonic,
and isokinetic). Knee spasticity was
measured bilaterally immediately before
and after the exercises using the pendulum
test to obtain a stretch reflex. The
measurements taken by Electrogoniometers
in the Pendulum test included the first
swing excursion, number of lower leg
oscillations, and duration of the oscillations.
The results of the study showed no increase
in quadriceps femoris spasticity after
maximum efforts.
PYSCHOLOGICAL
BENEFITS
In studies,
strength training has not only been
shown to have cardiovascular and neuromuscular-system
advantages, but strength training has
been shown to increase self-image, promote
active lifestyles, as well as encourage
socialization (McBurney,
Taylor, Dodd, & Graham, 2003).
Physical exercise is associated with
increased self-attitudes in people of
all ages who have physical and/or emotional
disorders (Ben-Shlomo
& Short, 1983). Winnick (2005)
states that for people with cerebral
palsy there must be attention paid to
psychological and social development.
A study, looking at the relationship
between quality of life and functional
status of young adults with cerebral
palsy (done by
Tarsuslu & Livanelioglu, 2010)
demonstrated that children with cerebral
palsy were more affected by parameters
related to physical condition, while
psychological and emotional aspects
were more important factors relating
to quality of life for adults with cerebral
palsy.
A study by
Allen, Dodd, Taylor, McBurney, &
Larkin (2004)
examined people with cerebral palsy,
and the positive and negative perceptions
of being involved in a strength-training
program. Ten participants were placed
in a ten-week group resistance-training
program. After the conclusion of the
study, the participants were interviewed
about how well they enjoyed that program.
The results of the interview showed
that the participants felt like his
or her strength had improved, and that
performing everyday tasks was easier,
but the main outcome for the participants
was the enjoyment and the social interaction
the program provided them with.
Negative
perceptions included short-term muscle
soreness, lack of monumental gains in
strength, and fatigue. Enjoyment plays
a vital component of adherence and sustainability
to strength training programs, which
can lead to increased function and socialization
(Allen et al.).
McBurney et al. (2003)
found similar psychological benefits
to strength training.
Contradicting
the studies by Allen et al. (2004)
and McBurney et al. (2003),
Dodd, Taylor, & Graham
(2004) found that an at-home
progressive strength-training program
had an inhibitory effect in regard to
social acceptance in children with cerebral
palsy. Seventeen children with spastic
diplegic cerebral palsy were recruited
to either take part in the strength
training or to be in the control group.
Self-concept measures were taken at
the beginning, right after the training,
and again six weeks after the training
as a follow-up. At baseline, six-weeks,
and at the follow-up, both of the groups
exhibited a positive self-concept. The
experimental group did show a decrease
in self-concept in the area of scholastic
competence and social acceptance after
the training, as well as at the follow-up.
Shields, Loy, Murdoch, Taylor, &
Dodd (2007)
found that children with cerebral palsy
do not have a reduced sense of Global
Self-worth even though they feel less
competent in some aspect of self-concept.
Self-concept may not be lower because
of the diagnosis of cerebral palsy,
but because of some other outside factors
(Shields et al.).
DISCUSSION
After reviewing
the literature concerning people with
cerebral palsy and the effects of strength
training on muscle strength, mobility,
gait function, spasticity, and self-concept,
there seems to be a positive correlation
between "progressive, task-oriented
strength training" in a community
setting and improvements in the dependent
variables. There is also evidence of
the relationship between lower body
strength training and motor functioning,
while there wasn't any evidence of strengthening
exercises increasing spasticity. It
is important that parents as well as
physical educators have an idea of where
weaknesses generally are in children
with cerebral palsy, and what exercises
will work on those areas of concern
(Appendix A.)
Looking into
the future, there should be more research
done in the area of progressive strength
training. One area that hasn't been
researched much is a progressive strength-training
program teamed with a stretching program.
Strength training and stretching are
two of the components of a complete
fitness program. Teaming the two together
may result in different outcomes.
page
2 >>
|

